The FDA Medical Device Approval Process
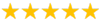
According to the Food and Drug Administration (FDA), more than 200,000 people are injured and as many as 2,000 are killed every year due to incidents linked to defective medical devices, such as hip and knee replacements, implants, transvaginal mesh, and contraceptive devices. In a great number of these cases, the risks are great enough that they may outweigh the potential benefits of the device, which is something patients must be aware of, if they are to be expected to make reasonable decisions regarding the use of these devices.
Over the last several years, there have been numerous reports suggesting that the FDA is placing patients at greater risk by approving many potentially invasive medical devices with roughly the same criteria that they use to approve crutches, wheelchairs, and hospital beds, which is essentially none. According to some reports, most of the moderate- to high-risk medical devices approved by the FDA in recent years did not include any sort of publicly-available scientific evidence or data that could be used to verify their efficacy and safety, even though the law requires that manufacturers of high-risk devices provide such evidence prior to approval, and that the FDA make the information publicly available.
The FDA uses three categories to classify medical devices according to risk. Class I devices include such low risk medical devices such as bandages, tongue depressors and arms legs, while Class II devices, which pose a moderate risk to patients include syringes, surgical instruments and hearing aids. Class III devices are considered high risk medical devices and are supposed to be subject to much greater scrutiny than Class I or Class II devices.
Unfortunately, too often high-risk Class III medical devices are being reviewed and approved by the FDA using a 510(k) process, which is a streamlined process that is supposedly meant to be used to approve Class I and Class II devices. However, manufacturers have apparently found a loophole of sorts. In order to qualify for a 510(k) review, the device manufacturers simply have to demonstrate that the new device is “substantially equivalent” to another device already on the market. The problem with this is, once one device is approved using this method, it becomes a “predictive” device that future 510(k) submissions can use as a reference point, which means a great many high-risk Class III devices are being approved by the FDA under the same standards as those reserved for lower-risk Class II devices, which means they’re less stringent, faster and far less expensive, all of which are good for manufacturers, but not so much for patients, since no proof of either effectiveness or safety is even necessary on the streamlined submission.
This is no small problem. According to a 2011 study published by a health research group, between 2005 and 2009, 113 medical devices were subject to recall and 80 of those made it to the market through the 510(k) process. Despite this record, according to another study in published just last year, between 2008 and 2012, of 50 new devices cleared by the FDA, only eight were actually “substantially equivalent” to devices that were cleared for market and of all previously cleared devices referenced, only about three percent had support through publicly available evidence.
Defective medical devices that are implanted inside the body can result in physical injuries that can sometimes be life-threatening and which can also cause excruciating pain and have a significant negative impact on the quality of life. The trauma often associated with these defective devices can lead to massive unforeseeable medical expenses and economic losses.